
Endurance Training/Cardiorespiratory
 photo")
Chimaobim E. Martin-Diala (he/him/his)
Graduate Research Assistant
University of South Carolina
Columbia, South Carolina, United States

Nestor Urrea, M.S.
Doctoral Student
University of South Carolina
Columbia, South Carolina, United States

Gianna F. Mastrofini, MS
Doctoral Student
University of South Carolina
Cayce, South Carolina, United States
Alexa J. Chandler
Doctoral Student
University of South Carolina
Columbia, South Carolina, United States

Blaine S. Lints, MS, CSCS,*D
Doctoral Student
University of South Carolina
York, South Carolina, United States

Emma E. Worley, MS
Doctoral Student
University of South Carolina
Cayce, South Carolina, United States

Sten O. Stray-Gundersen, PhD
Research Fellow
University of South Carolina - Sport Science Lab
Columbia, South Carolina, United States
Shawn M. Arent
Department Chair of Exercise Science
University of South Carolina
Columbia, South Carolina, United States
Cardiorespiratory fitness is a fundamental aspect of an athlete’s overall physical capability and is vital to sports performance. While indirect calorimetry via direct gas exchange is the gold standard method to measure maximal oxygen uptake (VO2max), this process requires specialized equipment and trained personnel to administer. Alternatively, field assessments offer a more accessible and cost-effective means for coaches to estimate VO2max. Despite these field tests being validated for the general population, there are limited data regarding the agreement between measured and predicted VO2max values in high-level soccer athletes.
Purpose: This study investigated the agreement between the multi-stage “yo-yo” fitness test (MSFT) and direct gas exchange analysis in determining VO2max. It was hypothesized the MSFT would overestimate VO2max due to the indirect nature of the valuation and fewer objective criteria for test termination.
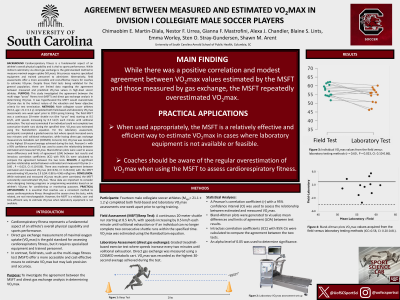
Methods: Male collegiate soccer athletes (N=14, age= 21.1±1.2 y) completed both field-based and laboratory VO2max assessments one week apart prior to 2024 spring training. The field MSFT was a continuous 20-meter shuttle run (the “yo-yo” test) starting at 8.5 km/h, with speeds increasing by 0.5 km/h each minute until volitional exhaustion. The test was terminated if an individual could not complete two consecutive shuttle runs during the specified time. VO2max was estimated using the Ramsbottom equation. For the laboratory assessment, participants completed a graded exercise test where speeds increased every two minutes until volitional exhaustion while having direct gas exchange measured via metabolic cart (COSMED, Concord, CA). VO2max was recorded as the highest 30-second average achieved during the test. Pearson’s r with a 95% confidence interval (CI) was used to assess the relationship between estimated and measured VO2max. Bland-Altman plots were used to assess mean differences and limits of agreement (LOA) between test results and intraclass correlation coefficients (ICC) with 95% CIs were calculated to compare the agreement between the two tests.
Results: A significant positive relationship existed between estimated and measured VO2max (r = 0.60, CI: 0.10-0.86, P = 0.023). There was moderate agreement between estimated and measured VO2max (ICC=0.58, CI: 0.20-0.81) with the MSFT overestimating VO2max by 2.9 (LOA: 0.88 to 4.96) ml/kg/min.
Conclusions: While estimated and measured VO2max results were correlated, the MSFT consistently overestimated VO2max. These data are important to consider when designing training programs or programming wearables based on an athlete’s VO2max for conditioning or monitoring purposes. PRACTICAL APPLICATIONS: It is essential that coaches use a consistent method to assess cardiorespiratory fitness throughout the season since the tests, while related, are not interchangeable. However, the MSFT is a reliable, cost- and time-efficient way to estimate VO2max when laboratory equipment is not available.
Acknowledgements:
This abstract was made possible in part by Grant Number T32-GM081740 from NIH-NIGMS. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIGMS or NIH.