
Speed/Power Development
Christopher J. Cleary, Jr., PhD
Graduate Teaching Assistant
Univeristy of Kansas
Lawrence, Kansas, United States
.jpg "Damjana V. Cabarkapa, PhD, CSCS, NSCA-CPT, TSAC-F,USAW photo")
Damjana V. Cabarkapa, PhD, CSCS, NSCA-CPT, TSAC-F,USAW
Graduate Teaching/Research Assistant
University of Kansas
Lawrence, Kansas, United States
Lexy N. Farrington
Undergraduate Research Assistant
University of Kansas
Lawrence, Kansas, United States
A. Wilkes Stephenson
Undergraduate Research Assistant
University of Kansas
Lawrence, Kansas, United States
Rachel E. Long
Research Assistant
University of Kansas Medical Center
Kansas City, Kansas, United States

Andrew C. Fry, PhD, CSCS*D, FNSCA*E
Professor
University of Kansas
Lawrence, Kansas, United States
Trent J. Herda
Professor
University of Kansas
Lawrence, Kansas, United States
Bryan G. Vopat
Orthopedic Surgeon
University of Kansas Medical Center
Kansas City, Kansas, United States
Ashley A. Herda
Assistant Professor
University of Kansas- Edwards Campus
Overland Park, Kansas, United States
Countermovement jumps and other similar sport-specific movements may have altered kinetics following anterior cruciate ligament injuries and reconstructive surgery (ACLR).
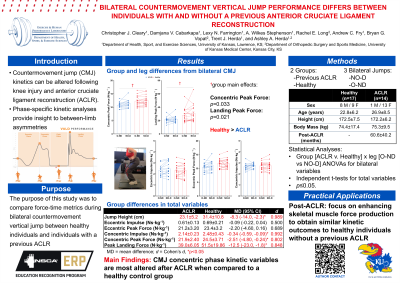
Purpose: This investigation compared force-time metrics during a maximal bilateral countermovement vertical jump between healthy individuals and individuals with a previous ACLR.
Methods: Thirty-one (22 female and 9 male; 17 healthy, 14 post-ACLR, mean age ±SD: 24.6±7.5 years) individuals volunteered to complete maximal bilateral countermovement jumps on a dual force plate system. Jump height, total (left + right) and per limb peak landing force relative to body mass, total and per limb relative concentric and eccentric impulse, and total and per limb relative concentric and eccentric peak force were assessed. Variables assessed separately on each limb were compared for the operative or non-dominant limb (O-ND) and the non-operative or dominant limb (NO-D). Separate mixed-factorial ANOVAs [group (ACLR vs. healthy) x leg (O-ND vs. NO-D)] assessed differences between groups and legs for each variable assessed on both legs at p≤0.05. Independent samples t-tests assessed differences in the bilateral variables with Cohen’s d effect sizes.
Results: There were no significant group x leg interactions for any variable assessed bilaterally (p=0.184-0.514) and no leg main effect for any variable (p=0.061-0.992). However, there was a significant group main effect for total relative concentric peak force and relative peak force. Follow-up tests indicated that the healthy group was greater than the ACLR group (mean difference ± standard error of the difference; p-value, d) for relative concentric peak force (1.28±0.57 N∙kg-1; p=0.033, d=0.810) and relative peak landing force (7.33±3.0 N∙kg-1; p=0.021, d=0.882) collapsed across legs. Further, the ACLR group had significantly lower bilateral countermovement jump height (8.35±2.95 cm; p=0.009, d=0.989), total relative concentric impulse (0.34±0.12 Ns∙kg-1; p=0.009, d=0.992), total relative concentric peak force (2.51±1.11 N∙kg-1; p=0.03, d=0.80) and total relative peak landing force (12.45±5.08 N∙kg-1; p=0.023, d=0.848) compared to the healthy group.
Conclusion: There were no unique effects of leg status on any variable assessed per limb despite cumulative bilateral differences in jump height, total relative concentric impulse, total relative concentric peak force, and total relative peak landing force. PRACTICAL APPLICATION: The group differences in outcome variables, such as jump height, may be explained by an individual’s ability to produce and apply force as indicated by the differences in concentric impulse and peak force. Training protocols for individuals after ACLR should focus on enhancing skeletal muscle force production during sport-specific tasks such as countermovement jumps to obtain similar kinetic outcomes to healthy individuals without a previous ACLR.
Acknowledgements: None.