
Endurance Training/Cardiorespiratory

Erica Schafer, MS
ORISE Post-Masters Research Fellow
U.S. Army Research Institute of Environmental Medicine
Natick, Massachusetts, United States
Jesse Stein
ORISE Post-Doctoral Research Fellow
U.S. Army Research Institute of Environmental Medicine
Natick, Massachusetts, United States
Christopher Chapman
ORISE Post-Doctoral Research Fellow
U.S. Army Research Institute of Environmental Medicine
Natick, Massachusetts, United States
Juliette Jacques
ORISE Research Fellow
U.S. Army Research Institute of Environmental Medicine
Natick, Massachusetts, United States
Brandon Roberts
Research Physiologist
U.S. Army Research Institute of Environmental Medicine
Natick, Massachusetts, United States
Adam Potter
Research Physiologist
U.S. Army Research Institute of Environmental Medicine
Natick, Massachusetts, United States
Karl Friedl
Chief Physiologist of the Army
U.S. Army Research Institute of Environmental Medicine
Natick, Massachusetts, United States

David P. Looney, PhD CSCS
Research Physiologist
Maximize Human Performance
Framingham, Massachusetts, United States
Maximal oxygen uptake (V̇O2max) is the criterion measure of cardiorespiratory fitness and is routinely assessed via a graded incremental treadmill protocol such as the Modified Astrand Running Test. However, speed-based running tests may be advantageous to reduce potential injuries, offset grade-dependent gait alterations, and for additional task-specificity for certain types of athletes.
Purpose: To determine: 1) the agreement between a speed-based V̇O2max incremental running test and a supramaximal verification test and 2) evaluate test-retest reliability of the speed-based incremental and verification tests.
Methods: Twelve healthy individuals (9 males, 3 females; mean ± SD; age, 24 ± 6 y; body mass, 73.8 ± 16.8 kg; height, 170 ± 8 cm) completed two laboratory visits that involved a speed-based incremental running test and a verification test (110% maximal incremental test speed). Test speeds were individualized based on each participant’s two-mile run time. Tests were performed until volitional exhaustion and were separated by 15 min of passive rest, while each laboratory visit was separated by ≥ 48 h of recovery. We tested the statistical equivalence between V̇O2max measured during the incremental and verification test at each visit as well as for tests between visits by evaluating whether the 90% confidence interval (CI) around the mean difference was within equivalence limits of ± 2.1 mL∙kg-1∙min-1. Test-retest reliability of the speed-based incremental and verification tests were quantified using interclass correlation coefficients (ICC).
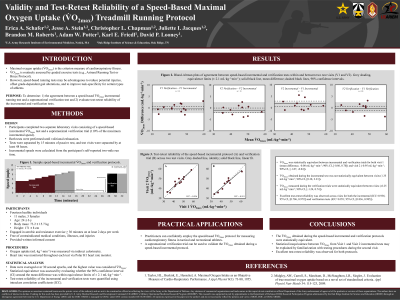
Results: V̇O2max was statistically equivalent between the incremental and verification tests across both visits (mean difference, −0.6 mL∙kg-1∙min-1; 90% CI, [−1.4, 0.2]). Similarly, V̇O2max was statistically equivalent when tests were compared between visits (0.7 mL∙kg-1∙min-1; 90% CI: −0.4, 1.9). Test-retest reliability was excellent for the speed-based incremental running test (ICC: 0.92, 90% CI, [0.75, 0.97]) but nearly perfect between the verification trials (ICC: 0.98, 90% CI, [0.96, 0.99]).
Conclusions: A speed-based incremental running test is a valid, reliable method for assessing V̇O2max in healthy adults. Repeating testing on a second visit yields only a minor improvement in V̇O2max. PRACTICAL APPLICATIONS: Practitioners can confidently employ the speed-based V̇O2max protocol for measuring cardiorespiratory fitness in tactical and recreational athletes.
The views expressed in this abstract are those of the authors and do not reflect the official policy of the U.S. Government, Department of Energy, Department of the Army, or Department of Defense.
Acknowledgements: None